Overview
The knee is a hinge joint: the femur (femur), tibia (tibia), and kneecap (patella) glide against one another on a smooth lining of cartilage, across three compartments. When the cartilage in all three wears away, what we call tricompartmental osteoarthritis, bone begins rubbing on bone, so walking, standing, and stairs become painful and the leg can start to bow or give out. This kind of arthritis is mechanical wear of the joint surface.
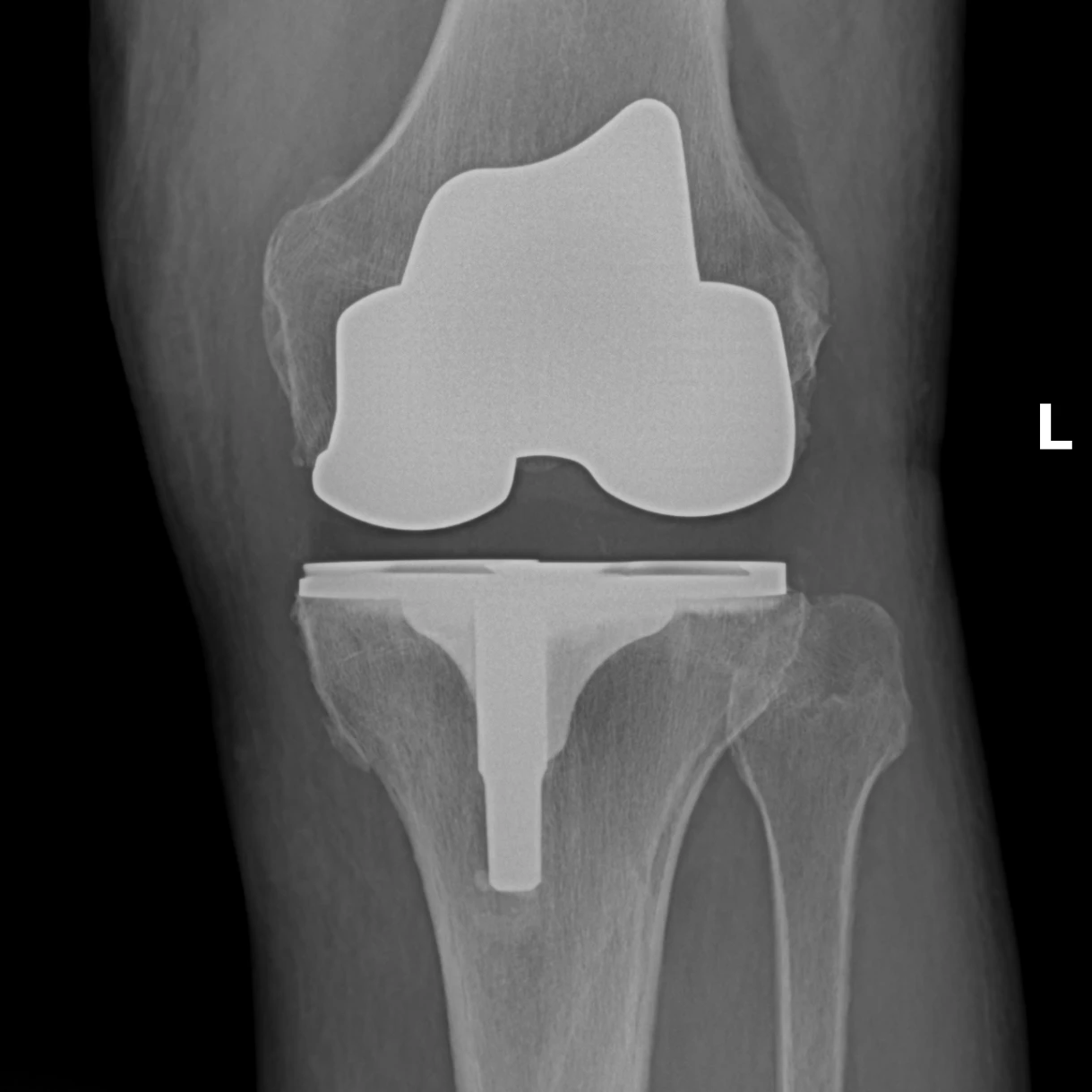
"Total knee replacement" is the standard name for this operation, but a more honest description is knee resurfacing. The knee itself is not removed. The damaged ends of the femur, tibia, and (usually) the back of the kneecap are shaved by a few millimeters and re-capped with metal and polyethylene. Most of the native bone, the ligaments on the sides of the knee, and the surrounding soft tissue are preserved. Many people arrive expecting a wholesale swap of the joint. It is a smaller operation than that word implies, and that is one reason recovery and long-term function are as good as they are.
How the Procedure Works
We remove the damaged cartilage and a measured layer of bone from the femur, tibia, and usually the back of the patella, no more than necessary, because bone removal is permanent. Metal components are cemented or press-fit onto the femur and tibia, with a polyethylene spacer between them. What most affects the outcome is not which implant is used; it is how carefully the knee is balanced and lined up. With trial parts in place, we test the knee as it bends and straightens and make small adjustments until it feels evenly snug in both positions. A knee that is well-balanced and properly lined up moves smoothly, carries weight evenly, and feels stable through the full range of motion. One that is not will hurt and wear unevenly no matter the implant brand.
When to Consider Total Knee Replacement
Total knee replacement is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Advanced Tricompartmental Arthritis
Cartilage loss across multiple compartments on weight-bearing X-rays, with daily pain and functional loss.
Exhausted Non-Operative Care
Failed extended course of anti-inflammatories, physical therapy, weight loss, bracing, and intra-articular injections.
Deformity or Instability
A leg that is increasingly bowed or knock-kneed, or a knee that buckles, both signal that the joint is no longer supporting the limb.
Treats: Knee Osteoarthritis
Risks & Why We Still Recommend It
Serious complications, such as an infection of the new joint, occur in fewer than 2 percent of patients. Every operation carries risk. This procedure is offered because the condition, when left untreated, can cause daily pain at rest and with walking, progressive deformity, and a leg that can no longer reliably bear weight. The decision to proceed weighs the risks of surgery against the limitations the condition places on daily function. Surgery does not remove risk; it addresses a problem that is otherwise progressive. Whether it is appropriate is determined for each patient in consultation with the surgeon.
The risks we discuss with you before total knee replacement include:
- bleeding and infection (including rare deep periprosthetic infection)
- anesthesia risk
- blood clot in the leg or lung, reduced with blood thinners, walking, and compression stockings after surgery
- stiffness, occasionally severe enough to require a procedure where the knee is gently moved through its range of motion while you are under anesthesia (manipulation under anesthesia)
- persistent pain from component malposition or soft-tissue imbalance
- periprosthetic fracture
- polyethylene or component wear over time, eventually requiring additional surgery
- rare nerve or blood-vessel injury behind the knee
The indication to proceed is end-stage arthritis across multiple knee compartments, with daily pain and functional loss that has not responded to a full course of non-operative care. If this operation is not right for you, we will not recommend it.
Recovery & What to Expect
sourced from AAOS patient guidanceYour surgeon will give you a recovery timeline specific to your procedure and healing. Physical therapy does the heavy lifting in the recovery period: the goal is a knee that straightens fully and bends far enough for stairs and chairs. On average, a replaced knee bends to about 115 degrees.
The replaced knee is built for a low-impact life. Unlimited walking, swimming, golf, biking, light hiking, and ballroom dancing are all realistic expectations. Most surgeons advise giving up running, jumping, and other high-impact sports permanently after a knee replacement.
The implant itself holds up well: more than 90 percent of modern total knee replacements are still working 15 years after surgery.
Frequently Asked
questions we hear in clinicIs the whole knee actually removed?
No. A more honest description of the operation is knee resurfacing. The damaged ends of the femur, tibia, and usually the back of the kneecap are shaved by a few millimeters and re-capped with metal and polyethylene. Most of the native bone, the ligaments on the sides of the knee, and the surrounding soft tissue are preserved.
How long will the new knee last?
More than 90 percent of modern total knee replacements are still working 15 years after surgery. What affects the outcome most is not the implant brand; it is the balancing and alignment work done during the operation.
When can I drive again?
Your surgeon will give you a recovery timeline specific to your procedure and healing, including when it is safe to return to driving and routine daily activities.
What activities are realistic afterward?
The replaced knee is built for a low-impact life: unlimited walking, swimming, golf, biking, light hiking, and ballroom dancing are all realistic expectations. Most surgeons advise giving up running, jumping, and other high-impact sports permanently after a knee replacement.
Am I too old for a knee replacement?
There are no absolute age restrictions. Candidacy is based on pain and function: daily pain, loss of walking tolerance, and X-ray findings together tell us whether the operation is the right step.
How serious are the risks?
Serious complications, such as an infection of the new joint, occur in fewer than 2 percent of patients. Every operation carries risk, and the reason we still recommend this one is that advanced arthritis, left untreated, causes daily pain and progressive deformity. The full picture is in the Risks section above.
Further Reading
External patient-education references and related OSI pages for additional background:




