Overview
When the rotator cuff cannot be repaired, a standard (anatomic) shoulder replacement will not work. Without the cuff, the ball will not stay centered in the socket. The reverse design solves that problem by swapping the two sides of the joint. The ball is fixed to the shoulder blade's socket (glenoid), and the new socket goes on the upper arm bone (humerus). This moves the joint's pivot point inward and downward. That gives the deltoid muscle the leverage to lift the arm even when the cuff cannot.
How the Procedure Works
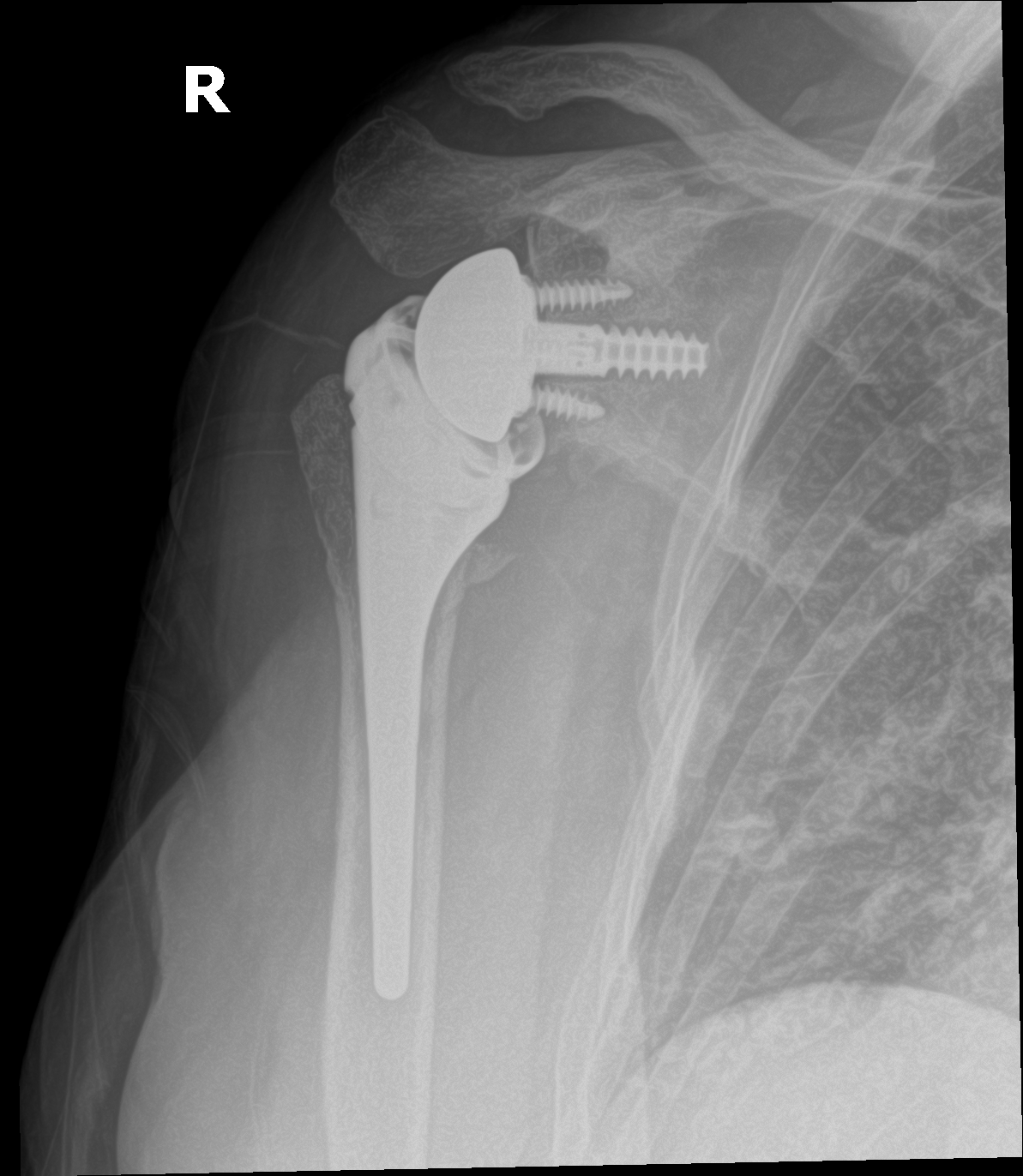
On the socket side, the most important step is fixing a metal baseplate solidly to the bone of the shoulder blade with screws. A loose baseplate is the most serious way this operation can fail. The round metal ball then locks onto the baseplate.
On the arm-bone side, we size the stem and set the height of the plastic socket to put the right amount of tension on the deltoid muscle. Too little tension and the joint can dislocate. Too much and you lose comfortable motion and risk a stress fracture of the shoulder blade (the acromion). We check motion and stability with trial parts before placing the final implants. After surgery, the deltoid muscle does all the lifting. The reversed design gives it the leverage the rotator cuff can no longer provide.
When to Consider Reverse Shoulder Replacement
Reverse shoulder replacement is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Rotator cuff arthropathy
Long-standing cuff failure leading to cuff-tear arthropathy. It is a pattern of arthritis that sets in when the shoulder runs for years without a working cuff.
Massive irreparable cuff tear
A huge cuff tear with pseudoparalysis. That means you cannot raise the arm above shoulder height on your own, even though the arm itself is not paralyzed.
Failed prior shoulder replacement
Revision from a failed anatomic replacement or fracture hemiarthroplasty.
Conditions This Treats
Risks & Why We Still Recommend It
Every operation carries risk. This procedure is offered because the condition, when left untreated, can cause a shoulder that cannot raise the arm, since arthritis together with a cuff that cannot be repaired leaves patients unable to reach a shelf or comb their hair. The decision to proceed weighs the risks of surgery against the limitations the condition places on daily function. Surgery does not remove risk; it addresses a problem that is otherwise progressive. Whether it is appropriate is determined for each patient in consultation with the surgeon.
The risks we discuss with patients before reverse shoulder replacement include:
- bleeding and infection (including rare deep periprosthetic infection)
- anesthesia risk
- dislocation of the reverse construct
- acromial or scapular-spine stress fracture
- component loosening over the long term
- scapular notching
- nerve irritation (axillary, transient)
- blood clot (rare in upper-extremity surgery)
We proceed for cuff-tear arthropathy, for a massive cuff tear with pseudoparalysis that cannot be repaired, or for complex shoulder fractures in older patients when fixing the bone is not an option. If you don't need this operation, we won't recommend it.
Frequently Asked
questions we hear in clinicWhy reverse the ball and socket?
When the rotator cuff cannot be repaired, a standard replacement will not keep the ball centered in the socket. Swapping the two sides moves the joint's pivot point inward and downward, which gives the deltoid muscle the leverage to lift the arm even when the cuff cannot.
Is this the same as a standard shoulder replacement?
No. In a standard (anatomic) replacement the ball stays on the arm side. In the reverse design, the ball is fixed to the shoulder blade's socket and the new socket goes on the upper arm bone.
What lifts my arm if the rotator cuff is gone?
After surgery, the deltoid muscle does all the lifting. The reversed design gives it the leverage the rotator cuff can no longer provide.
What is the most serious way this operation can fail?
A loose baseplate on the socket side. That is why the most important step on that side is fixing the metal baseplate solidly to the bone of the shoulder blade with screws.
Who is this operation for?
The typical candidates are cuff-tear arthropathy, a massive cuff tear with pseudoparalysis (you cannot raise the arm above shoulder height on your own, even though the arm is not paralyzed), and revision of a failed prior shoulder replacement.
What are the main risks?
The risks we discuss include dislocation of the reverse construct, a stress fracture of the acromion or scapular spine, component loosening over the long term, scapular notching, transient nerve irritation, and infection.
Further Reading
External patient-education references and related OSI pages for additional background:




