
Overview
what it is and why it matters
"Knee arthritis" covers more than one condition. The common one, and the subject of this page, is osteoarthritis (OA): the slow, mechanical wearing-out of the cartilage that caps the joint surfaces. Post-traumatic arthritis follows the same mechanical path, set off by an earlier fracture or ligament injury, and is treated the same way once it sets in. Inflammatory and crystal-related arthritis, such as rheumatoid arthritis and gout, is a different, systemic disease diagnosed and managed by rheumatology; OSI refers out when a systemic cause is suspected.
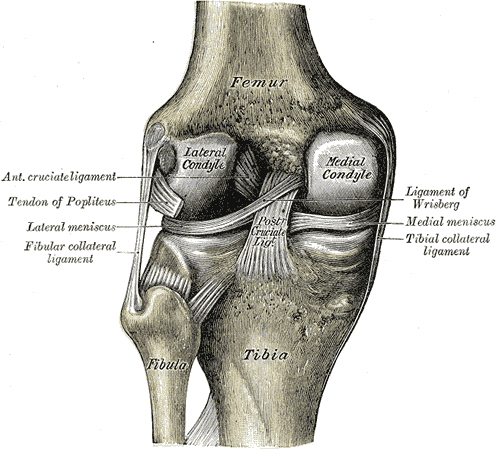
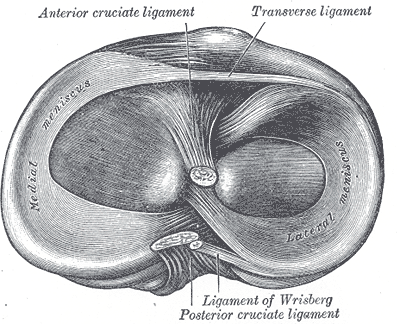
Cartilage has no nerves, so a knee can look worn on X-ray well before it aches. The pain comes from the other structures around it: the bone beneath the worn cartilage, the inflamed joint lining, and the bony spurs the joint builds at its rim as it loses stability. Most arthritis builds up over decades from use, genetics, and body weight. Some cases trace to a specific cause: a meniscus tear, an ACL rupture, a fracture into the joint surface, or alignment that overloads one side of the knee.
The knee has three compartments: the inner side (the medial compartment), the outer side (the lateral compartment), and the joint behind the kneecap (the patellofemoral compartment). During level walking the joint carries three to four times your body weight, and even higher loads at the kneecap joint on stairs. Cartilage and the meniscus cushions spread that load; as cartilage thins, force concentrates on shrinking patches of bone, the joint inflames, and spurs form. The medial side carries more load in most knees, so it tends to wear first, which is why many people grow progressively bow-legged (varus); a knock-kneed (valgus) leg wears the lateral side first instead. Losing a meniscus, to a tear or an earlier meniscus surgery, accelerates cartilage loss on that side. Every pound of body weight adds roughly four pounds of force across the knee with each step, which is why weight has the most direct effect of anything you control.
Symptoms
what patients describeMost patients describe a deep ache rather than a sharp pain. Many notice the gel phenomenon: the knee stiffens after sitting still and takes a few minutes of walking to loosen. Morning stiffness, when it occurs, tends to be brief, often under half an hour; stiffness that drags on much longer is worth mentioning to your provider. Stairs, especially going down, are often harder than level ground, and the ache can build over the day. Some people hear grinding or feel a catch as worn surfaces meet, particularly when a degenerative meniscus tear is also present. Swelling or a sense of warmth after activity is common.
As OA advances, your leg may visibly bow or turn knock-kneed as one compartment wears faster than the other, swelling can become more constant, and deep bending (kneeling, squatting, sitting cross-legged) gets harder. Pain that wakes you at night is a later signal worth an evaluation. These patterns overlap with other knee conditions, so they point toward an exam, not a self-diagnosis.
Diagnosis & Evaluation
exam first, imaging secondYour provider examines the knee, checks its alignment and motion, and looks for the catching, grinding, and tenderness that point to worn cartilage. Weight-bearing X-rays are the standard images: front-to-back, side, and kneecap views taken while you stand. Standing matters, because films taken off your feet make the joint space look wider than it is under load. These views show how much cartilage space remains and how the alignment has shifted.
MRI is not required to diagnose OA. It is reserved for specific questions: a meniscus tear in a younger patient, possible bone damage from poor blood supply, or soft-tissue problems X-rays cannot show. If your provider suspects a systemic or inflammatory cause rather than mechanical wear, you are referred to rheumatology for that workup. The diagnosis rests on the exam and these images together, read by your provider.
How We Treat It
what we try first, in orderMost arthritic knees are managed without surgery. The aim is plain: take load off the cartilage, calm the inflammation, and strengthen the muscles that protect the joint. The treatments below are grouped the way we usually introduce them, the foundation first, then medication and injections, and they build on each other rather than replace one another.
The foundation: what you control
Body weight is the largest factor you control; given the load multiplier above, even modest weight loss meaningfully unloads the joint. Low-impact conditioning (cycling, swimming, elliptical) keeps fitness up without grinding the worn surfaces together. Quadriceps strengthening, the muscles on the front of the thigh, acts as a shock absorber for force before it reaches the cartilage. Physical therapy builds these into a routine you can keep.
Pain control without surgery
Oral anti-inflammatories (ibuprofen, naproxen, meloxicam) ease the inflammatory part of the pain, used intermittently when kidney, stomach, and heart health allow. Topical diclofenac rubbed over the knee gives similar relief with less systemic exposure, and suits mild-to-moderate flares.
Injections, used judiciously
Cortisone injection. A single intra-articular corticosteroid shot can interrupt a pain cycle and buy weeks to months, useful as a bridge while therapy takes hold or a surgery is planned. Repeated injections are limited, because frequent steroid can harm cartilage.
Hyaluronic acid (viscosupplementation). A lubricating gel injection that coats the worn surfaces. Sometimes considered after the standard measures (activity changes, physical therapy, anti-inflammatories, and a cortisone shot) have been tried. The evidence is mixed, strongest in the knee but limited overall. It is offered self-pay.
Platelet-rich plasma (PRP). Growth factors concentrated from your own blood and injected into the joint, considered after the standard options. Not covered by insurance; offered self-pay.
Bracing
Unloader bracing. A hinged brace that shifts weight off the worn compartment onto the healthier side. Works best when only the medial or only the lateral compartment is involved and the ligaments are intact.
When Surgery Is Considered
when function no longer respondsThe decision to operate rests on how much the knee is interfering with your life, not on the X-ray alone. Surgery is considered when non-surgical care no longer gives adequate relief: pain that wakes you at night, activities that matter being given up, or daily pain medication needed to get through the day. Which operation fits depends on where the arthritis sits and how your leg is aligned, and is decided together with your surgeon.
Total knee replacement
Resurfaces all three compartments with metal and plastic bearing surfaces. The standard operation when arthritis involves most of the joint and non-surgical care no longer controls the pain.
Learn about this procedure →Partial knee replacement
For arthritis confined to one compartment with intact ligaments. Resurfaces only the worn side and preserves the rest of the knee.
Learn about this procedure →High tibial osteotomy
Realigns the tibia to shift weight off the worn compartment. An option for younger, active patients whose alignment overloads one side, to delay a replacement.
Learn about this procedure →If non-surgical care is not enough, these procedures can address this condition:
Frequently Asked
questions we hear in clinicDo I need an MRI to diagnose knee arthritis?
Usually not. Osteoarthritis is diagnosed from the exam and weight-bearing X-rays read together by your provider. An MRI is reserved for specific questions, such as a meniscus tear in a younger patient, possible bone damage from poor blood supply, or soft-tissue problems X-rays cannot show.
My X-ray looks bad. Does that mean I need surgery?
Not on its own. The decision to operate rests on how much the knee is interfering with your life, not on the X-ray alone. Surgery is considered when non-surgical care no longer gives adequate relief, for example pain that wakes you at night, activities that matter being given up, or needing daily pain medication to get through the day.
Will losing weight really help my knee?
Yes, more than almost anything else you control. Every pound of body weight adds roughly four pounds of force across the knee with each step, so even modest weight loss meaningfully unloads the joint. Pairing it with low-impact conditioning and quadriceps strengthening protects the cartilage further.
How often can I get a cortisone shot?
A single cortisone injection can interrupt a pain cycle and buy weeks to months, which is useful as a bridge while physical therapy takes hold or a surgery is planned. Repeated injections are limited, because frequent steroid can harm cartilage.
What is the difference between a total and a partial knee replacement?
A total knee replacement resurfaces all three compartments and is the standard operation when arthritis involves most of the joint. A partial knee replacement is for arthritis confined to one compartment with intact ligaments; it resurfaces only the worn side and preserves the rest of the knee.
Is this the same as rheumatoid arthritis or gout?
No. This page is about osteoarthritis, the mechanical wearing-out of cartilage. Inflammatory and crystal-related arthritis, such as rheumatoid arthritis and gout, is a different, systemic disease diagnosed and managed by rheumatology. When a systemic cause is suspected, OSI refers out for that workup.
Providers Who Treat Knee Osteoarthritis
Treated by the OSI orthopedic team across all six offices. Meet the team →
Further Reading
authoritative sourcesExternal patient-education references and related pages for additional background: