Overview
The hip is a ball-and-socket joint. The ball is the top of the femur (femoral head). The socket (acetabulum) is part of the pelvis. A smooth cartilage lining lets the two glide. That lining can wear away from osteoarthritis, inflammatory arthritis, bone death (avascular necrosis), or damage after an old injury. Once it does, bone grinds on bone and every step hurts. Total hip replacement resurfaces both sides of the joint with a smooth metal-and-plastic implant.
How the Procedure Works
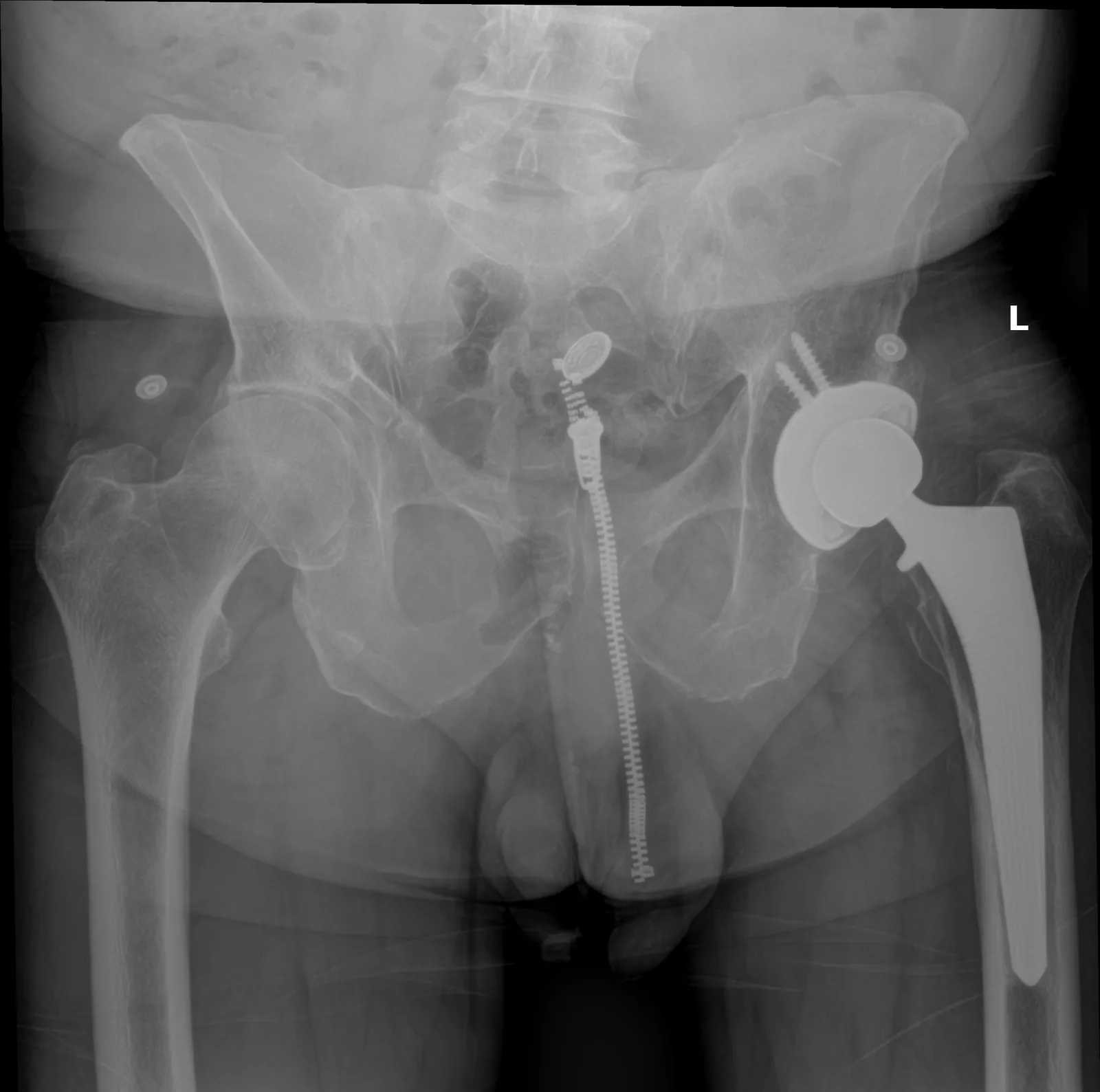
We reach the hip through the back of the buttock. We split the large buttock muscle along its fibers and temporarily release the small rotator muscles beneath it. At the end of surgery, those small muscles are repaired back to bone. That repair greatly lowers the risk of the new hip dislocating, compared to leaving them unattached. We then remove the worn femoral head, which gives a clear view of the socket. We shape the socket and confirm the cup angle on live X-ray (fluoroscopy). Then we seat the metal shell and click in the plastic liner. On the other side, we prepare the canal of the femur and seat the stem. The final ball head goes on last. We measure leg lengths with care during surgery and confirm them on X-ray. Being off by more than a centimeter is one of the most common reasons patients are unhappy after a hip replacement. Careful measurement during surgery largely prevents it.
When to Consider Posterior Total Hip Replacement
We generally offer posterior total hip replacement when your symptoms, your imaging, and a full course of non-surgical care all point the same way. The typical picture includes:
Pain that limits daily life
Hip pain that gets in the way of walking, stairs, or sleep despite a full course of anti-inflammatory medicine, therapy, and activity changes.
Radiographic arthritis
X-rays that show lost joint space, bone spurs (osteophytes), bone death, or wear from an old injury, in a pattern that matches your symptoms.
Exhausted non-operative care
Non-surgical care has not worked. That includes weight loss, low-impact exercise, NSAIDs, and injections into the joint.
Good surgical candidate
Your medical conditions are well controlled and there is no active infection. Your bone quality and anatomy can hold an implant.
Conditions This Treats
Risks & Why We Still Recommend It
Every operation carries risk. This procedure is offered because the condition, when left untreated, can cause groin and thigh pain with every step, lost motion, and a steady loss of the ability to stand, walk, and sleep in comfort. The decision to proceed weighs the risks of surgery against the limitations the condition places on daily function. Surgery does not remove risk; it addresses a problem that is otherwise progressive. Whether it is appropriate is determined for each patient in consultation with the surgeon.
The risks we discuss before posterior total hip replacement include:
- bleeding and infection (including rare deep periprosthetic infection)
- anesthesia risk
- blood clot in the leg or lung, reduced with blood thinners, walking, and compression stockings after surgery
- dislocation, particularly in the early recovery phase
- leg-length discrepancy
- sciatic nerve injury (rare)
- periprosthetic fracture
- component loosening or wear over time
The reason to proceed is end-stage hip arthritis with daily pain and lost function that has not improved with non-surgical care. Patients who do not need this operation do not get it.
Frequently Asked
questions we hear in clinicWhat does "posterior" mean for my surgery?
We reach the hip through the back of the buttock, splitting the large buttock muscle along its fibers and temporarily releasing the small rotator muscles beneath it. At the end of surgery those small muscles are repaired back to bone.
Will the new hip dislocate?
Dislocation is one of the risks we discuss, particularly in the early recovery phase. Repairing the small rotator muscles back to bone at the end of surgery greatly lowers that risk compared to leaving them unattached.
Will my legs end up the same length?
We measure leg lengths with care during surgery and confirm them on live X-ray before closing. Being off by more than a centimeter is one of the most common reasons patients are unhappy after a hip replacement, and careful measurement during surgery largely prevents it.
Do I need this operation, or can I wait?
We generally offer it when your symptoms, your imaging, and a full course of non-surgical care all point the same way. That means hip pain getting in the way of walking, stairs, or sleep despite a full course of anti-inflammatory medicine, therapy, activity changes, weight loss, and injections. Patients who do not need this operation do not get it.
What wears a hip out in the first place?
The smooth cartilage lining of the ball-and-socket can wear away from osteoarthritis, inflammatory arthritis, bone death (avascular necrosis), or damage after an old injury. Once it does, bone grinds on bone and every step hurts.
Further Reading
Outside reading we trust, plus related OSI pages:




