Overview
The meniscus, the C-shaped cartilage cushion between the femur (femur) and tibia (tibia), is tethered to the tibia at its front and back attachments, its roots. When a root detaches, the meniscus is functionally uncapped and extrudes out of the joint, no longer distributing load across the cartilage. Untreated, this accelerates arthritis as quickly as removing the entire meniscus (a total meniscectomy) would.
How the Procedure Works
We pass two heavy sutures through the detached meniscus root using a locking stitch pattern, then drill a tunnel through the tibia aimed precisely at the normal attachment spot. For the most common tear (the back of the inner meniscus), that spot sits just in front of where the PCL, the knee's back ligament, attaches to the tibia. Tunnel placement is the most critical step: even a small error in position shifts where the meniscus rests and keeps it from properly sharing load across the joint. The sutures are pulled through the tunnel and tied over a small button on the front of the tibia with the knee nearly straight. Before closing, we probe the meniscus to confirm it has seated back in the joint rather than buckling outward, and we check that it tracks normally with rotation. If the leg bows inward, we address that at the same time. A root repair in a bow-legged knee will be overloaded unless the alignment is corrected alongside it.
When to Consider Meniscus Root Repair
Meniscus root repair is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
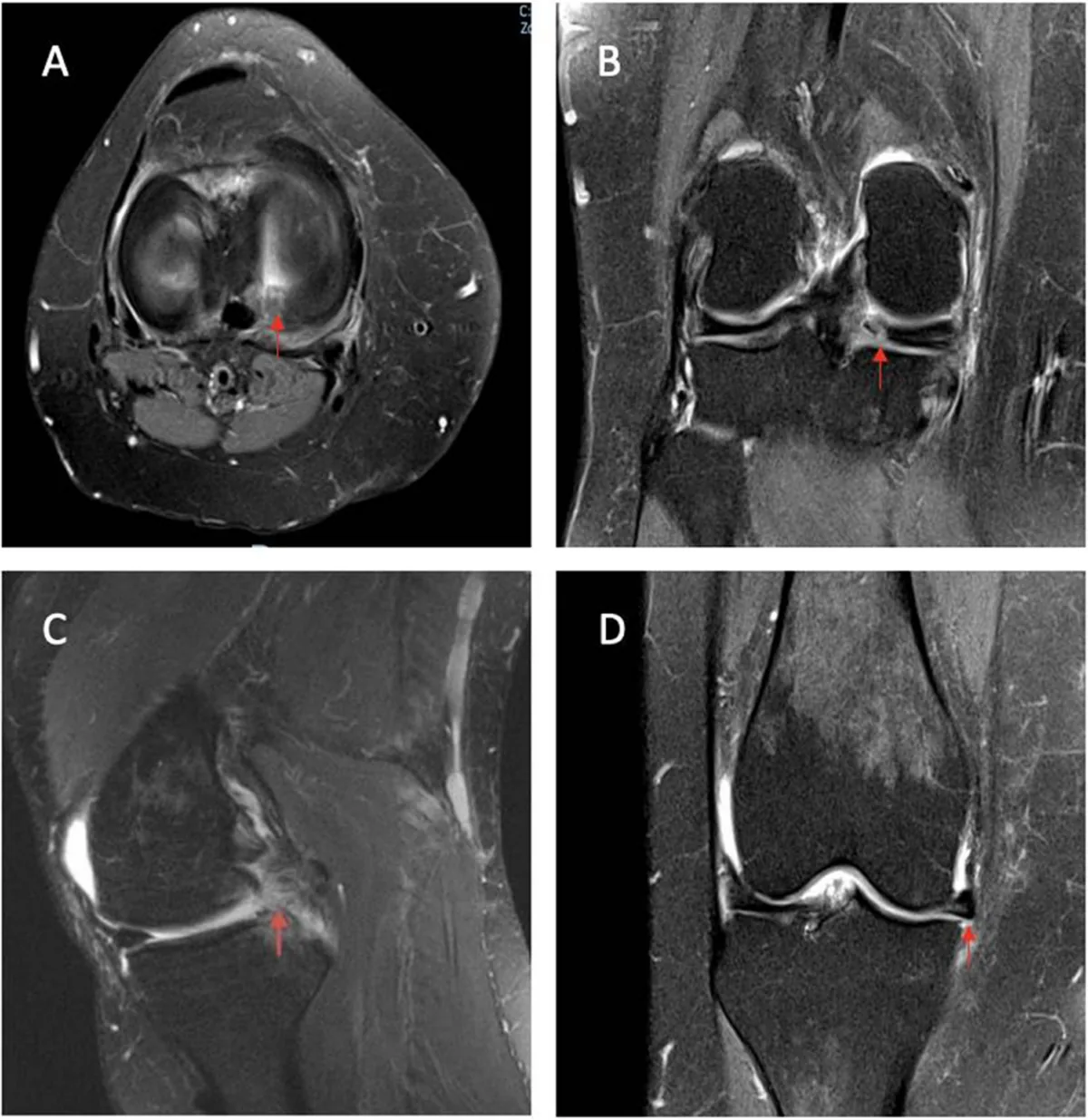
Acute medial root tear
Especially common in middle-aged patients after a deep squat or minor injury, presenting as sudden medial knee pain.
Active patients without end-stage arthritis
Best outcomes occur before the underlying cartilage has worn through.
Preserved alignment
A neutral or correctable axis that won't overload the repaired meniscus.
Treats: Meniscus Tear
Risks & Why We Still Recommend It
Every operation carries risk. This procedure is offered because the condition, when left untreated, can cause rapid loss of meniscal function, since a root tear behaves like a total meniscectomy and accelerates arthritis on that side of the knee. The decision to proceed weighs the risks of surgery against the limitations the condition places on daily function. Surgery does not remove risk; it addresses a problem that is otherwise progressive. Whether it is appropriate is determined for each patient in consultation with the surgeon.
The risks we discuss with you before meniscus root repair include:
- bleeding and infection
- anesthesia risk
- stiffness
- failure of the root to heal back to bone
- suture pull-out or tunnel-related issues
- blood clot in the leg or lung
The indication to proceed is a recent or sub-acute posterior root tear in a knee that still has preserved cartilage and alignment worth protecting. If the operation is not right for you, we will say so.
Frequently Asked
questions we hear in clinicWhat makes a root tear different from a regular meniscus tear?
The meniscus is tethered to the tibia at its front and back attachments, its roots. When a root detaches, the whole meniscus is functionally uncapped: it extrudes out of the joint and no longer distributes load across the cartilage.
What does a root tear feel like when it happens?
The most common pattern is an acute tear at the back of the inner meniscus, especially in middle-aged patients after a deep squat or minor injury, presenting as sudden inner-knee pain.
What happens if I leave it alone?
Untreated, a root tear behaves like removal of the entire meniscus and accelerates arthritis on that side of the knee just as quickly. That is the trade we weigh against the risks of surgery.
How is the root reattached?
Two heavy sutures are passed through the detached root with a locking stitch, then pulled through a tunnel drilled in the tibia, aimed precisely at the normal attachment spot, and tied over a small button on the front of the tibia. Before closing, we probe the meniscus to confirm it has seated back in the joint and tracks normally with rotation.
What if I am bow-legged?
We address that at the same time. A root repair in a bow-legged (varus) knee will be overloaded unless the alignment is corrected alongside it.
Who gets the best results from this repair?
Active patients without end-stage arthritis, with a recent or sub-acute tear and preserved alignment. Best outcomes occur before the underlying cartilage has worn through.
Further Reading
External patient-education references and related OSI pages for additional background:




