Overview
what it is and why it mattersCarpal tunnel syndrome happens when the median nerve, the nerve that gives your thumb, index, middle, and half of your ring finger their feeling and fine movement, gets squeezed where it passes through a narrow channel at the base of your palm (the carpal tunnel). It is the most common nerve-pinching condition in the upper limb, affecting roughly 3 to 4 percent of people at some point in life. Women get it two to three times more often than men, and it becomes more common with age.
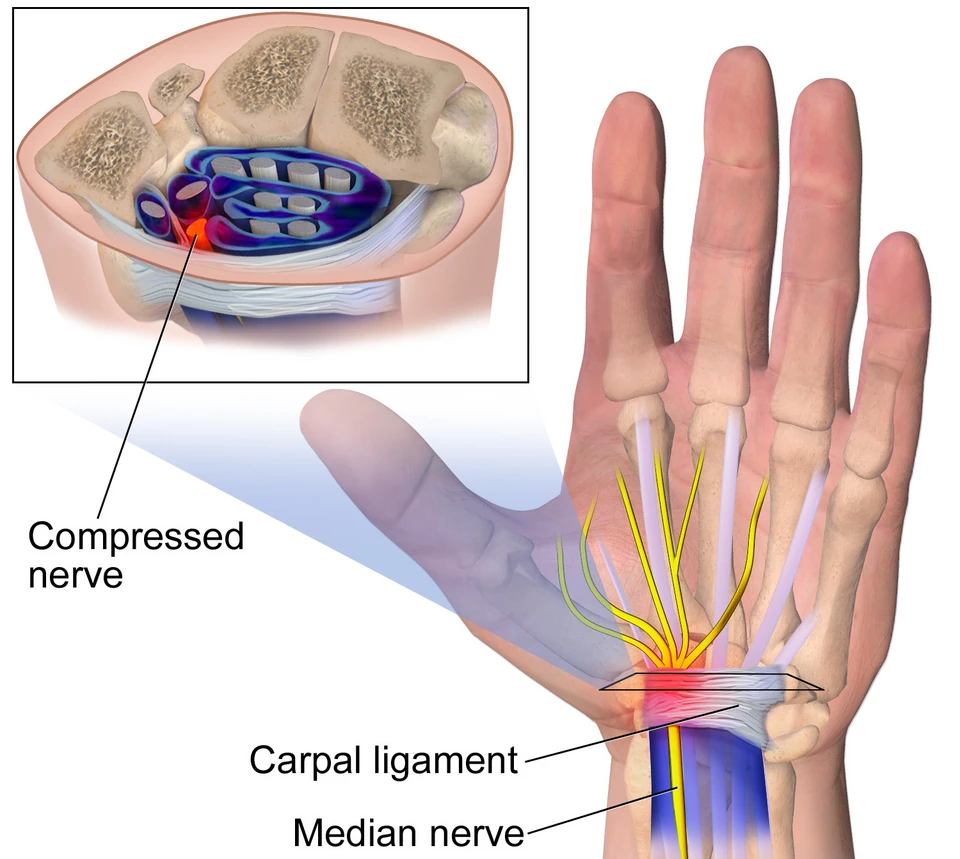
The carpal tunnel is a small channel at the base of your palm: the wrist bones make the floor and walls, and a tough band of tissue called the transverse carpal ligament forms the roof. Inside, the median nerve shares that narrow space with nine tendons that bend your fingers. Anything that raises pressure inside the tunnel, such as swelling of the tendon linings, fluid retention, a cyst, or holding your wrist sharply bent for long stretches, can squeeze the nerve. Mild compression first irritates the nerve's outer insulation; long-standing severe compression damages the nerve fibers themselves. That is why mild cases often improve with non-surgical care, while advanced cases, especially when the muscle at the base of the thumb has visibly shrunk, may not fully recover even after a successful release.
In most people there is no single cause. Things that make it more likely include carrying extra weight, pregnancy, a previous wrist fracture, and work or hobbies that involve long stretches of gripping or vibration (assembly-line work, knitting for hours, motorcycles, power tools). A systemic medical condition sometimes contributes; when one is suspected, your primary-care provider or a rheumatologist evaluates and manages that side of it, while OSI addresses the mechanical compression at the wrist.
Symptoms
what patients describeThe hallmark of carpal tunnel syndrome is numbness and tingling in your thumb, index finger, middle finger, and the thumb-side half of your ring finger, precisely the territory the median nerve supplies. Most people notice it first at night: you wake up with pins and needles in your hand, and shaking it out often brings quick relief. The reason is positional, your wrist naturally curls inward as you sleep, which kinks the already-tight tunnel and raises the pressure on the nerve.
During the day the same pattern shows up whenever your wrist stays bent for a stretch, gripping a steering wheel, holding a phone to your ear, reading a book in bed. Over time the numbness creeps in more easily and takes longer to clear. You may start fumbling with buttons, dropping small objects, or struggling to pick up a coin from a flat surface, the nerve controls the fine pinch between your thumb and fingertips, and when its signal weakens, those precision tasks are the first to go.
In advanced cases the muscle pad at the base of your thumb (the thenar eminence) visibly flattens and shrinks, a sign that nerve fibers have been damaged, not just irritated. If numbness has become constant or you notice that flat spot forming, those are reasons to move evaluation up rather than wait.
Diagnosis & Evaluation
exam plus electrodiagnostics when neededMost of the time the diagnosis is made right in the exam room with a focused physical exam of the hand and wrist. Your surgeon will also check the fine sensation in your fingertips and the strength of the muscles at the base of your thumb to track how severe the compression is over time.
When the diagnosis isn't clear-cut, or when surgery is on the table, your surgeon may order electrodiagnostic studies, a combination of nerve conduction studies (small electrical pulses that measure how quickly the signal travels through the nerve) and EMG (a thin needle in the muscle to see how it's responding). Together these confirm carpal tunnel, grade how severe it is, and rule out other causes like a pinched nerve in the neck (cervical radiculopathy). Ultrasound can also show swelling of the median nerve right where it enters the tunnel and is useful in selected cases.
How We Treat It
what we try first, in orderNon-surgical care is the first step for mild-to-moderate cases, especially when the thumb muscles still look and feel normal. Three things have solid evidence behind them: a wrist splint worn at night, an injection of corticosteroid into the tunnel, and a short course of oral anti-inflammatory pills. The strongest short-term combination is the splint plus the injection. The measures below are listed in the order we usually introduce them.
First-Line Measures
1
Night-Time Wrist Splint
A wrist splint worn at night holds your wrist straight, preventing the sustained bend that drives the nighttime numbness. Many patients see meaningful improvement after just a few weeks of consistent use.
2
Activity and Ergonomic Modification
Adjusting your keyboard and mouse position, taking short breaks during long stretches of typing or gripping, and avoiding holding your wrist sharply bent, small daily changes that add up.
3
Corticosteroid Injection
A single injection of corticosteroid into the carpal tunnel, guided in real time by ultrasound for accuracy, gives lasting relief to about one in three patients, and meaningful short-term relief to most. The response is also a useful clue: a strong response predicts that surgery will work well if symptoms come back later.
Anti-Inflammatory Pills, Used Briefly
A short course of over-the-counter anti-inflammatory pills can quiet symptoms for a stretch, and is one of the three measures with evidence behind it. It works best alongside the night splint and, when used, the injection rather than on its own.
When Surgery Is Considered
reliable relief for recalcitrant or severe casesCarpal tunnel release, surgery to cut the band of tissue that forms the roof of the tunnel and create more space for the nerve, is considered when the case is already severe at the first visit (visible thumb-muscle wasting, constant numbness, or markedly abnormal nerve tests), when a real attempt at non-surgical care has not worked, or when symptoms come right back after a corticosteroid injection. Release very reliably relieves the tingling and night symptoms. Recovery of strength and full sensation in advanced cases is less predictable and depends on how healthy the nerve was going in.
Recovery after release is usually straightforward. Night symptoms and tingling typically improve first, often early in recovery. A deep ache at the base of the palm, "pillar pain," is common for a period and gradually resolves, and grip strength returns more slowly as the hand is used normally. Recovery of sensation and thumb strength tracks how severe the compression was before surgery; patients with long-standing, advanced disease and visible thenar atrophy may have residual deficits even after a successful release. Your OSI provider advances activity based on the hand's response, not a fixed calendar.
If non-operative care is not enough, this procedure can address the condition:
Frequently Asked
questions we hear in clinicWhy is it worse at night?
The reason is positional. Your wrist naturally curls inward as you sleep, which kinks the already-tight tunnel and raises the pressure on the nerve. That is why most people notice it first at night, waking up with pins and needles, and why shaking the hand out often brings quick relief.
Can carpal tunnel get better without surgery?
Often, yes. Non-surgical care is the first step for mild-to-moderate cases, especially when the thumb muscles still look and feel normal. A night-time wrist splint, ergonomic changes, and a corticosteroid injection all have evidence behind them, and the strongest short-term combination is the splint plus the injection.
Do I need a nerve test?
Not always. Most of the time the diagnosis is made right in the exam room. Electrodiagnostic studies (nerve conduction studies and EMG) are ordered when the diagnosis isn’t clear-cut or when surgery is on the table. They confirm carpal tunnel, grade how severe it is, and rule out other causes such as a pinched nerve in the neck.
How well does a cortisone injection work?
A single injection of corticosteroid into the tunnel gives lasting relief to about one in three patients, and meaningful short-term relief to most. The response is also a useful clue: a strong response predicts that surgery will work well if symptoms come back later.
Will surgery fix the numbness and weakness?
Carpal tunnel release very reliably relieves the tingling and night symptoms. Recovery of strength and full sensation in advanced cases is less predictable and depends on how healthy the nerve was going in. Patients with long-standing, advanced disease and visible thumb-muscle wasting may have residual deficits even after a successful release.
What is recovery after surgery like?
Recovery after release is usually straightforward. Night symptoms and tingling typically improve first, often early on. A deep ache at the base of the palm, called “pillar pain,” is common for a period and gradually resolves, and grip strength returns more slowly as the hand is used normally. Your OSI provider advances activity based on the hand’s response, not a fixed calendar.
Providers Who Treat Carpal Tunnel Syndrome
hand & upper-extremity team


Further Reading
authoritative sourcesExternal patient-education references and related OSI pages for additional background: