Overview
The knee has three separate compartments: the inner side (medial), the outer side (lateral), and the joint behind the kneecap (patellofemoral). Arthritis does not always wear all three at once. When cartilage loss is limited to one compartment, a partial knee replacement resurfaces only the damaged area and leaves everything else alone. Surgeons also call it a unicompartmental knee arthroplasty (UKA).

That difference matters for how the knee feels and works after surgery. A total knee replacement removes and replaces all three, including the cruciate ligaments, no matter which parts were worn. A partial replacement keeps your ACL, your PCL, the healthy cartilage elsewhere in the knee, and more of your own bone. The knee keeps its normal, ligament-guided motion. Patients often say it feels more like their own joint and less like a mechanical part.
Isolated arthritis shows up most often on the inner side of the knee. That side accounts for the vast majority of partial replacements. Outer-side and kneecap replacements are less common. They are still reasonable options when the wear is clearly limited to those areas and the rest of the joint is healthy.
Partial knee replacement is not the right operation for every patient with knee arthritis. To be a good candidate, your pain should come from one part of the knee. Your ligaments must be intact and working. Any change in your leg's alignment must be correctable. When those conditions are met, the operation usually means a faster recovery, smaller incisions, and less blood loss than a total replacement. Long-term pain relief is excellent.
How the Procedure Works
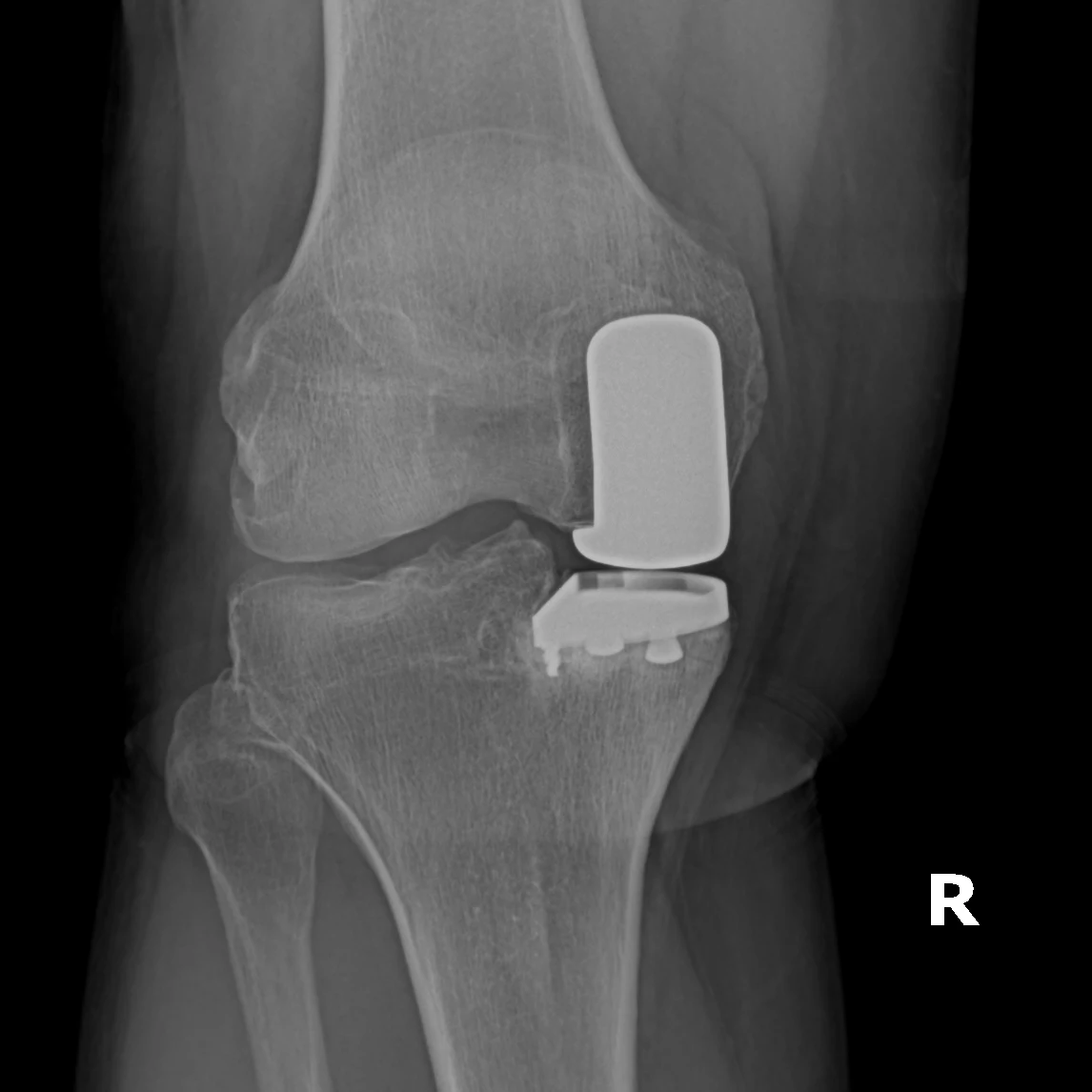
We resurface only the worn compartment, most often the inner side of the knee, with a smaller metal-and-plastic implant. Both cruciate ligaments, the other side of the joint, and the kneecap joint are left entirely alone. Choosing the right patient is the most important factor in how well this operation works. The ACL must be working, because it drives the natural gliding motion the partial implant relies on. The leg's alignment must correct passively on exam. The rest of the joint must have healthy cartilage. During surgery, we size the implant and set its slope to match your own knee. The goal is a part that joins the knee's normal motion rather than fighting it. Because the ligaments are kept, the knee keeps its sense of position (proprioception). That is why patients often say a partial feels more like their own knee than a total does.
When to Consider Partial Knee Replacement
Partial knee replacement is usually a fit when your symptoms, your imaging, and your response to non-surgical care all point the same way. The typical picture includes:
Single-compartment arthritis
Cartilage loss limited to the inner or outer compartment, confirmed on standing (weight-bearing) X-rays.
Intact ligaments
A working ACL and PCL. The ligaments must still steady the knee for a partial replacement to work.
Correctable deformity
A bow-legged or knock-kneed alignment (varus or valgus) that straightens passively on exam. That suggests the rest of the knee is still healthy.
Treats: Knee Osteoarthritis
Risks & Why We Still Recommend It
Every operation carries risk. This procedure is offered because the condition, when left untreated, can cause daily pain in one part of the knee and a steady loss of the active, low-intensity life these patients want back. The decision to proceed weighs the risks of surgery against the limitations the condition places on daily function. Surgery does not remove risk; it addresses a problem that is otherwise progressive. Whether it is appropriate is determined for each patient in consultation with the surgeon.
The risks we discuss with patients before partial knee replacement include:
- bleeding and infection
- anesthesia risk
- blood clot in the leg or lung
- progression of arthritis into the other compartments, eventually converting to a total knee
- the implant loosening or its plastic liner wearing out, which can require additional surgery
- persistent pain if patient selection or alignment is off
- a break in the bone around the implant (rare)
The reason to proceed is arthritis limited to the inner or outer compartment, with intact ligaments and good alignment, in someone who fits the checklist above. If the operation is not right for you, we will say so.
Frequently Asked
questions we hear in clinicWhat is the difference between a partial and a total knee replacement?
A total knee replacement removes and replaces all three compartments, including the cruciate ligaments, no matter which parts were worn. A partial replacement resurfaces only the damaged compartment and keeps your ACL, your PCL, the healthy cartilage elsewhere in the knee, and more of your own bone.
Will it feel like my own knee?
Because the ligaments are kept, the knee keeps its normal, ligament-guided motion and its sense of position (proprioception). Patients often say a partial feels more like their own joint and less like a mechanical part.
Am I a candidate?
The main factors are cartilage loss limited to one compartment confirmed on standing X-rays, a working ACL and PCL, and a bow-legged or knock-kneed alignment that straightens passively on exam. Partial knee replacement is not the right operation for every patient with knee arthritis.
Is recovery easier than a total knee replacement?
When the candidacy conditions are met, the operation usually means a faster recovery, smaller incisions, and less blood loss than a total replacement. Long-term pain relief is excellent.
What if arthritis spreads to the rest of my knee?
That is one of the risks we discuss before surgery: progression of arthritis into the other compartments can eventually mean converting to a total knee replacement.
Further Reading
Outside reading we trust, plus related OSI pages:




